Blood cancer & marrow failure · Hyderabad & Telangana
Bone Marrow Transplant in Hyderabad
A bone marrow transplant — also called a stem cell transplant, or BMT — replaces the blood-forming cells that a blood cancer or marrow-failure condition has stopped making. At CION the indicative cost is ₹8–15 lakh. And a transplant is not always the answer — many people are treated well without one. This page tells you, honestly, when a transplant is usually needed and when it usually is not.
Indicative ₹8–15 lakh · a real estimate for your case
A second opinion before you commit to anything
Follow-up close to home across Telangana & AP
★★★★★Rated 4.8/5 · 800+ Google reviews
35+ centres, close to home
17+ oncologists, one team
Second opinion before you commit
Aarogyasri & insurance help
BP
Written by Dr. Basudev Pokhrel, Haematologist (MBBS, Tribhuvan University · MD Immunohaematology & Blood Transfusion, JIPMER · Post-Doctoral Fellowship in Clinical Haematology, CMC Vellore). Medically reviewed by Dr. N. Kiranmayee, Medical Oncologist, DM (Medical Oncology). · Reviewed 14 July 2026
Cost & coverage
What a bone marrow transplant costs in Hyderabad Indicative
Bone marrow transplant in Hyderabad is commonly quoted at ₹10 lakh to ₹35 lakh, depending on the centre and the type of transplant. At CION, the indicative range is ₹8 lakh to ₹15 lakh. These figures are indicative and are not a quotation.
Indicative cost by type of transplant — CION Cancer Clinics, Hyderabad
Haploidentical / unrelated Half-match or registry donor
Assessed case by case
About 6–8 weeks
When there is no matched sibling donor
Indicative cost estimator
Pick your situation for an indicative range, then request an exact estimate for your case.
Indicative range
₹8,00,000 – ₹11,00,000
for an autologous transplant, general room, self-pay
Figures are indicative only and not a quotation. Half-matched and unrelated-donor transplants are assessed individually and cost more. Aarogyasri / PMJAY may cover eligible treatment at empanelled centres, subject to eligibility. Your actual cost depends on your diagnosis, donor and recovery.
Almost no hospital tells you this, and it is the part that catches families out — particularly families travelling in from a district.
Accommodation in Hyderabad for an attendant, typically four to six weeks — someone has to stay.
Travel, for the patient and for the family.
Lost earnings — for the patient, and usually for the family member attending.
Medication after discharge, which continues for months.
Follow-up blood counts and transfusions after discharge — these, at least, CION can do at your nearest centre.
Free consultation
Talk to a haematologist first — free
Bring your reports, or come in for a fresh evaluation. Before you commit to a transplant, it is worth finding out whether you need one — and what it would really cost in your case.
An honest second opinion with full molecular review
A real cost estimate for your case — not a brochure range
Aarogyasri / PMJAY & insurance guidance
First things first
What bone marrow actually does
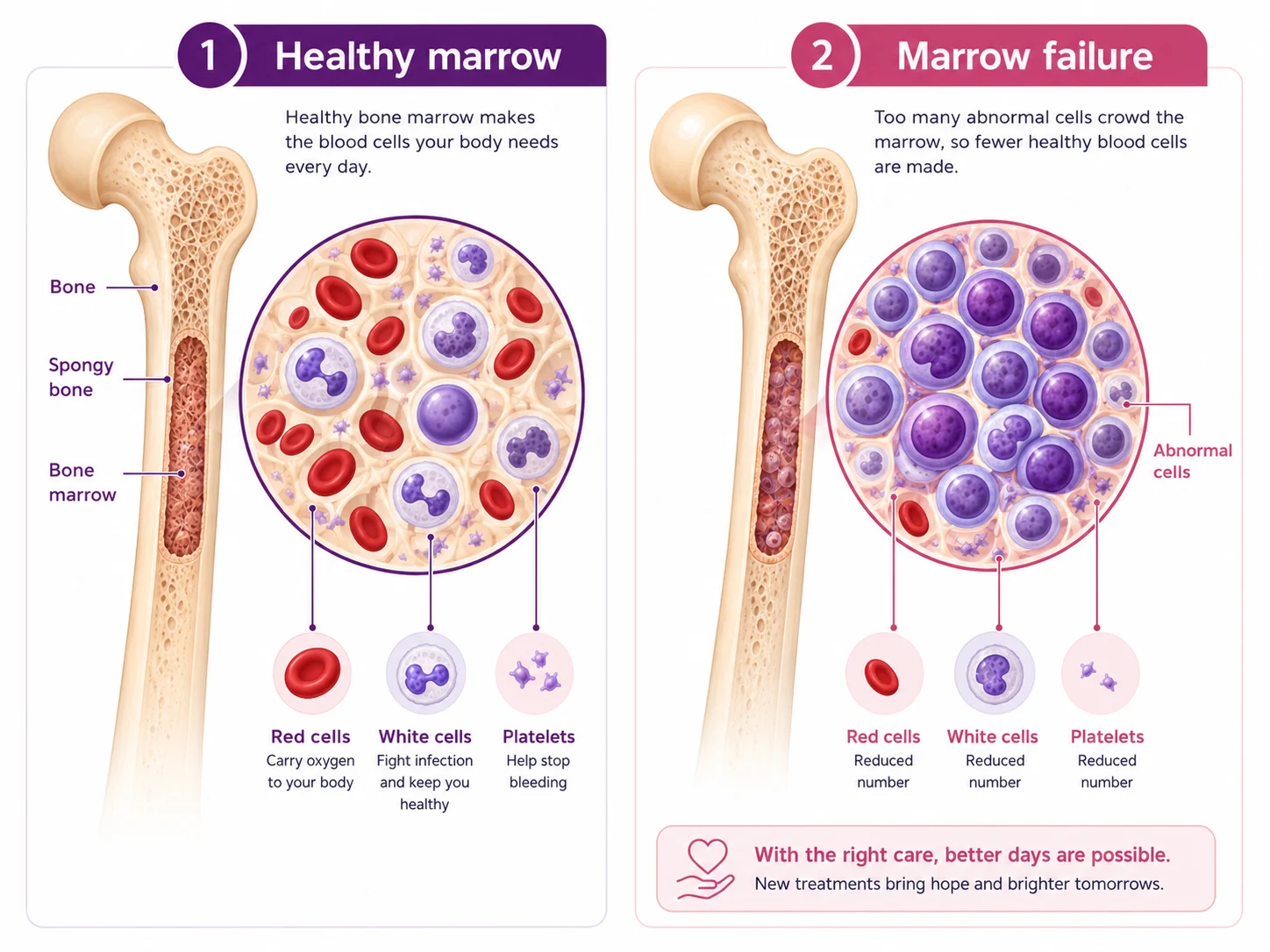
Bone marrow is the spongy tissue inside your bones, and it is a factory. It makes the three things your blood is built from: red cells that carry oxygen, white cells that fight infection, and platelets that stop bleeding.
In a blood cancer, that factory starts producing abnormal, immature cells that crowd out the healthy ones — which is why people become tired, bruise easily and catch infection after infection. A transplant is a way of replacing the factory.
Almost everything else on this page follows from that one idea. It is why the old marrow has to be cleared before new cells go in, why blood counts fall to nothing for a couple of weeks afterwards, and why recovery is measured in months rather than days — a factory takes time to start up.
Healthy marrow makes red cells, white cells and platelets. In blood cancer, abnormal cells crowd them out.
The honest question first
Do you actually need a transplant?
Often, no. A transplant is not the standard treatment for every blood cancer, and it is not something to agree to simply because it has been mentioned. Whether it is right for you depends on your exact subtype, your genetic and molecular results, and how the disease has responded to treatment so far. Here is where a transplant usually sits for each condition — and where it usually does not.
AML · depends on risk group
Acute myeloid leukaemia
Not a foregone conclusion. Whether transplant is advised depends on the leukaemia's genetic risk group and how completely it responds to first treatment. Many favourable-risk patients in remission never need one — which is exactly why the molecular and cytogenetic results matter so much.
ALL · higher-risk or relapsed
Acute lymphoblastic leukaemia
Many people — children especially, and many adults — are treated with chemotherapy alone and never need a transplant. It is generally considered for higher-risk genetics, disease that does not clear with initial treatment, or a relapse.
CML · rarely needed today
Chronic myeloid leukaemia
If you have been told you need a transplant for CML, get a second opinion. Most people today take a daily tablet at home and live many years with the disease well controlled. Transplant is now reserved for the few who don't respond to targeted therapy.
Lymphoma · usually only if it returns
Lymphoma (Hodgkin & non-Hodgkin)
Most lymphomas are treated with chemotherapy and immunotherapy, and most people never need a transplant at all. Where it comes in, it is usually an autologous transplant considered when the lymphoma returns or does not respond.
Myeloma · common, but after drug therapy
Multiple myeloma
An autologous transplant is a standard part of care for many who are fit for it — but it comes after an initial course of drug therapy, and it aims to deepen and prolong remission, not to cure. It can give years of good-quality life.
Aplastic anaemia · often first choice
Aplastic anaemia
Not a cancer — the marrow simply stops producing enough cells. For a younger patient with severe disease and a matched sibling, allogeneic transplant is frequently the preferred first treatment rather than a last resort.
Thalassaemia · age matters
Thalassaemia major
For a child, transplant is the only treatment that can end lifelong transfusions and iron chelation. Outcomes are meaningfully better when done young, before iron overload accumulates — one of the few situations where delay itself carries a cost.
MDS · for higher-risk disease
Myelodysplastic syndrome
Lower-risk MDS is often managed supportively for years. For higher-risk MDS, allogeneic transplant is the only treatment aimed at eliminating the disease — but it is demanding, and whether someone can tolerate it depends on age and organ function.
This is general information, not a diagnosis or a recommendation for your case. Only a haematologist who has read your actual reports can tell you whether a transplant is right for you. If one has been recommended and you are unsure, a second opinion is a reasonable thing to ask for — not an act of disloyalty to your doctor.
The tests that decide whether a transplant is right — and safe
Before any transplant, two things are confirmed: that a transplant is genuinely the right treatment for your disease, and that your body can withstand it. That means blood tests, a marrow biopsy, molecular and cytogenetic testing, HLA typing for you and potential family donors, and checks of heart, lung, liver and kidney function. Book any part of the work-up below.
Diagnostic & evaluation services we offer — book any of these:
Bone marrow biopsy
A small marrow sample to confirm the diagnosis and check how the disease is responding.
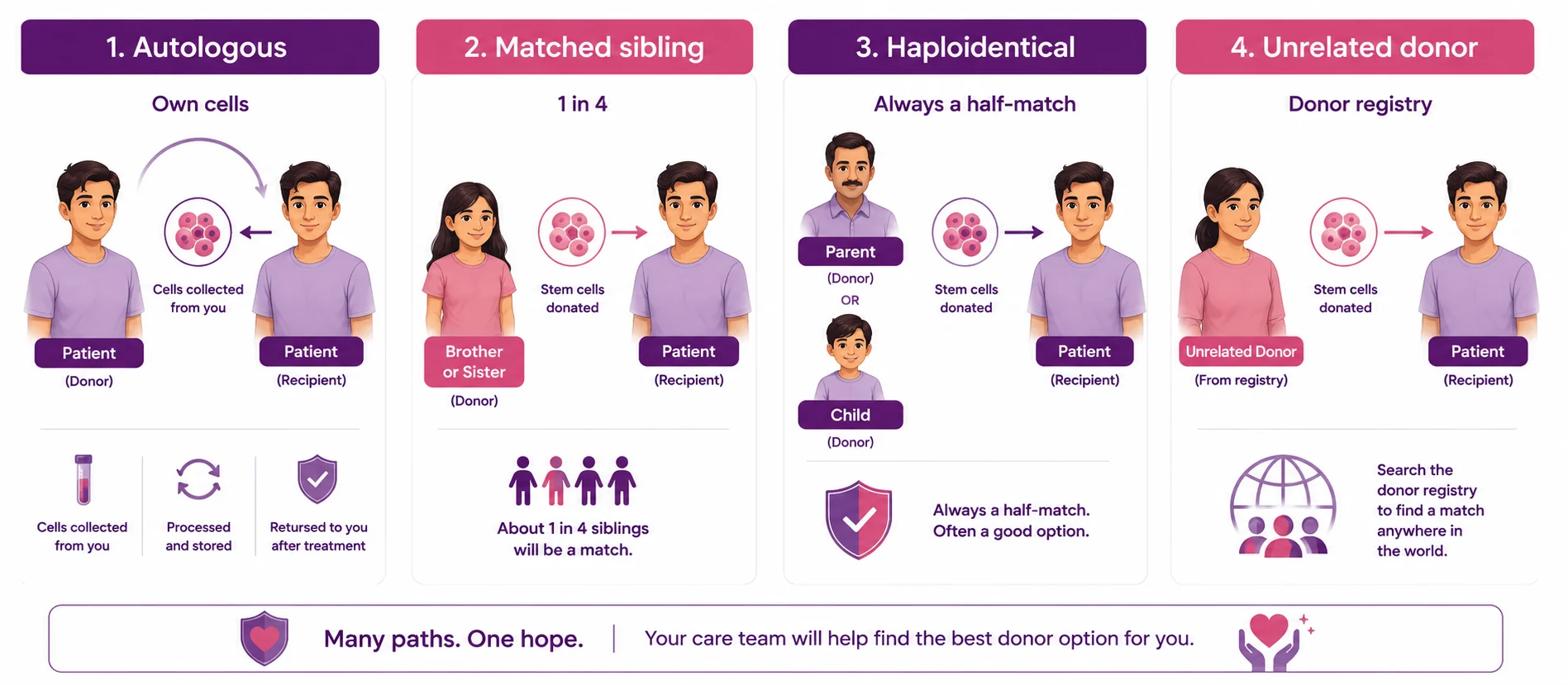
Transplants are named after where the stem cells come from. That single fact determines the cost, the risks, the length of stay, and whether you need to find a donor at all.
The four routes at a glance. Each one is explained below.
Autologous — your own cells
Your own stem cells are collected before high-dose treatment, stored, and given back afterwards. There is no donor to find and no risk of the graft attacking your body. Mainly used in multiple myeloma and lymphomas that have returned.
Allogeneic — a matched sibling
Stem cells come from a brother or sister who is a full HLA match. A full sibling has roughly a one in four chance of matching. The donor's immune system also helps attack any remaining cancer — part of why this works.
Haploidentical — a half-match
Stem cells come from a parent or a child, who is always at least a half-match. This is the option that changed everything: a family without a matched sibling is no longer a family without a donor.
Unrelated donor or cord blood
Where no family donor is available, a matched unrelated donor may be found through a registry, or stem cells may come from banked umbilical cord blood. The search takes longer, and the cost is higher.
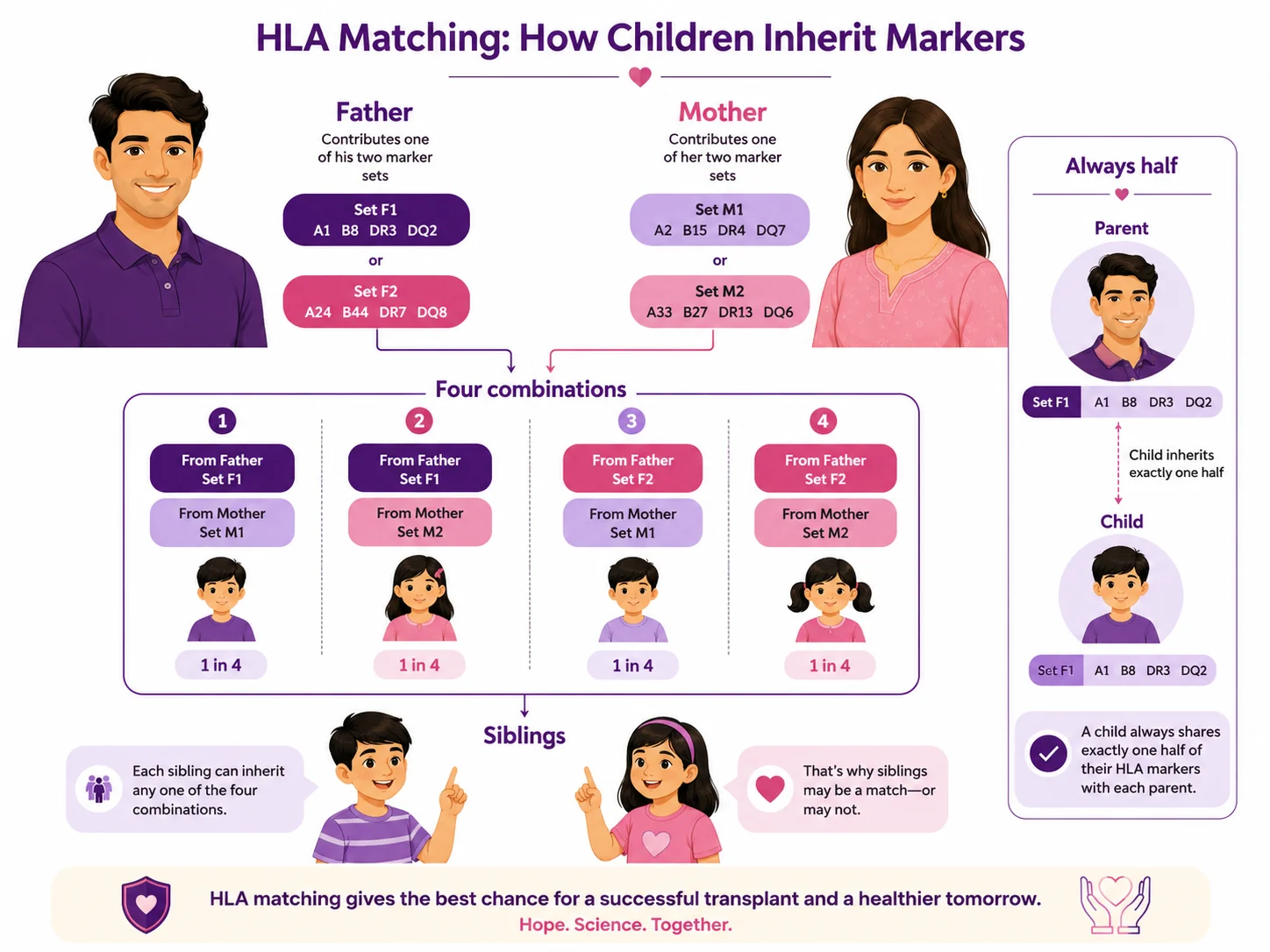
Why a sibling match is 1 in 4 — and why a parent always works
Everybody quotes the one-in-four figure; almost nobody explains it. Your HLA type — the set of markers a donor has to match — comes in two halves. You inherit one half from your father and one half from your mother. Each parent has two halves to give, so there are four possible combinations a child can end up with. Two siblings match fully only when they happen to draw the same combination — hence one in four.
But look at what the same arithmetic says about parents. Since you got exactly half your HLA type from your father and half from your mother, a parent is always a half-match. So is a child. Not usually. Not if you are lucky. Always. That is why haploidentical transplant matters so much, and why "we have no matching brother or sister" is not the end of the conversation families believe it to be.
HLA is inherited in halves — one from each parent. Four combinations means siblings match about one time in four; a parent or child is always a half-match.
What actually happens
What actually happens — start to finish
The transplant itself is not a surgery. There is no operation, no scalpel and no general anaesthesia. The stem cells go in through a soft tube into a vein, much like a blood transfusion — the patient is awake, sitting up, and it takes a few hours.
What makes people unwell is the conditioning chemotherapy in the days beforehand, and the weeks of very low immunity afterwards — not the transplant.
No operating theatre. The stem cells are infused through a central line — it looks like a blood transfusion, and the cells find their own way to the bone.
1
Evaluation
1–2 weeks. Tests confirm a transplant is right for you and that your body can withstand it.
2
HLA typing
1–3 weeks. A blood test for you and potential family donors. The step families dread — and it is only a blood test.
3
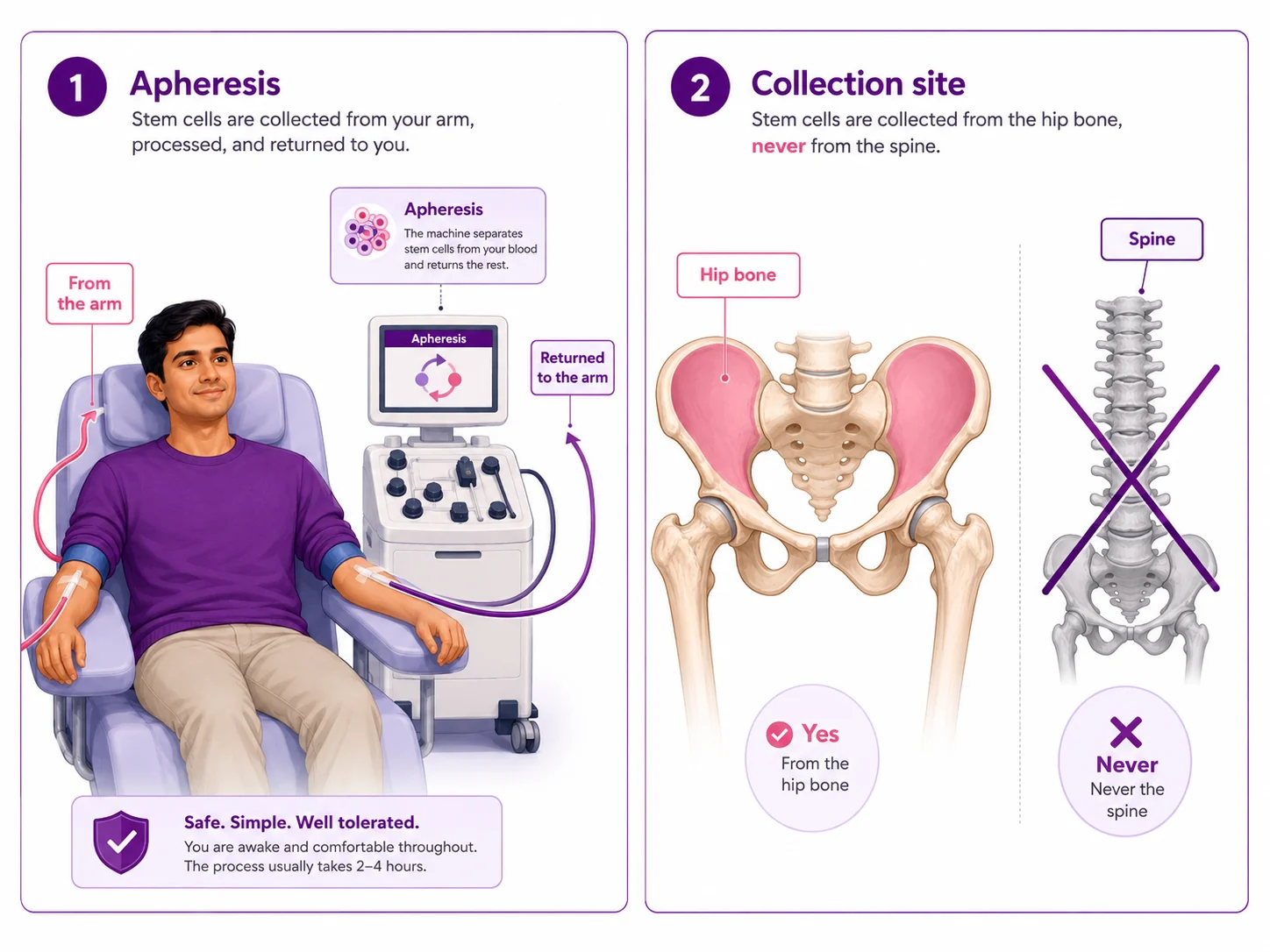
Collection
1–5 days. Usually apheresis — blood out of one arm, through a machine, back into the other. No surgery.
4
Conditioning
5–10 days. High-dose treatment clears the old marrow to make room. The hardest part of the process.
5
Day 0 — infusion
A few hours. The stem cells go in through the central line. Patients are often surprised how ordinary it feels.
6
Engraftment
2–4 weeks in protected isolation, while the new cells settle in and start producing blood.
7
Discharge & follow-up
3–6 months and beyond. Home, with careful monitoring as the immune system rebuilds.
Only one step on that list is outside your control, and it is the one families get stuck on: finding a donor. That is the next question — and it is where the most damaging misunderstanding in this whole process lives.
If your family member is asked to donate
Where stem cells actually come from
Across Telangana, families believe bone marrow is taken from the spine, and that donating leaves a person permanently weak — unable to lift, unable to farm, unable to work. Siblings refuse to be tested because of it.
It is not true, and it has cost people their lives.
Stem cells are collected from the arm by apheresis, or from the hip bone. Never from the spine.
“They take it from the spine.”
No. Nothing goes into the spine, ever. Most donors today give stem cells through apheresis — blood drawn from one arm, passed through a machine that separates out the stem cells, and returned through the other arm. It is closer to donating platelets than to any operation. Where actual marrow is collected, it is drawn from the hip bone with a needle, under anaesthesia.
“He'll be weak for life.”
No. The body replaces donated stem cells within a few weeks — that is what these cells do. Donors are typically back to normal activity within days of apheresis, and within a week or two after a marrow harvest. Farmers farm. Labourers work. There is no permanent loss of strength.
“It will affect her fertility or marriage.”
No. Donating stem cells does not affect fertility, does not affect the ability to have children later, and leaves no lasting mark. An unmarried sister who donates is in exactly the same position afterwards as before.
“Donating might give him cancer.”
No. Donating stem cells does not cause cancer and does not increase a donor's risk of it. The donor's marrow simply makes more cells to replace the ones given.
Who in your family could be a donor?
A brother or sister
About a 1 in 4 chance of a full match
Each full sibling has roughly a one-in-four chance of being a complete HLA match; with more than one sibling, the odds that at least one matches go up. Finding out costs nothing more than a blood sample. Testing is not consent to donate — it is simply information.
A parent or a child
Always at least a half-match
A parent or a child is always a half-match — arithmetic, not luck. Half-matched (haploidentical) transplant is now well established and performed routinely. If you have a living parent or an adult child, you have a potential donor.
Both available
Test the siblings first
A fully matched sibling is generally the preferred donor, so siblings are typed first. If none match — and three times in four, none will — a parent or child is always a half-match. With both available, you are very unlikely to be left without a donor at all.
Neither / not sure
Still not out of options
Harder, but not the end. Matched unrelated donors can be found through registries, and umbilical cord blood is another source. It costs more and takes longer, so book a haematology consultation now rather than concluding from a search result that nothing can be done.
Your evaluation, haematology care, transplant decision and follow-up are led by CION's own team. The transplant itself is performed at accredited partner transplant centres in Hyderabad, under a formal arrangement, with the same haematology team managing your case throughout. Book a consult for any of these.
Book a consultation for any of these:
Autologous transplant
Your own stem cells collected, stored and returned — mainly for myeloma and relapsed lymphoma. No donor needed.
A bone marrow transplant is a serious undertaking with real risks, and you should be told them plainly. Anyone who presents it as routine is not being straight with you.
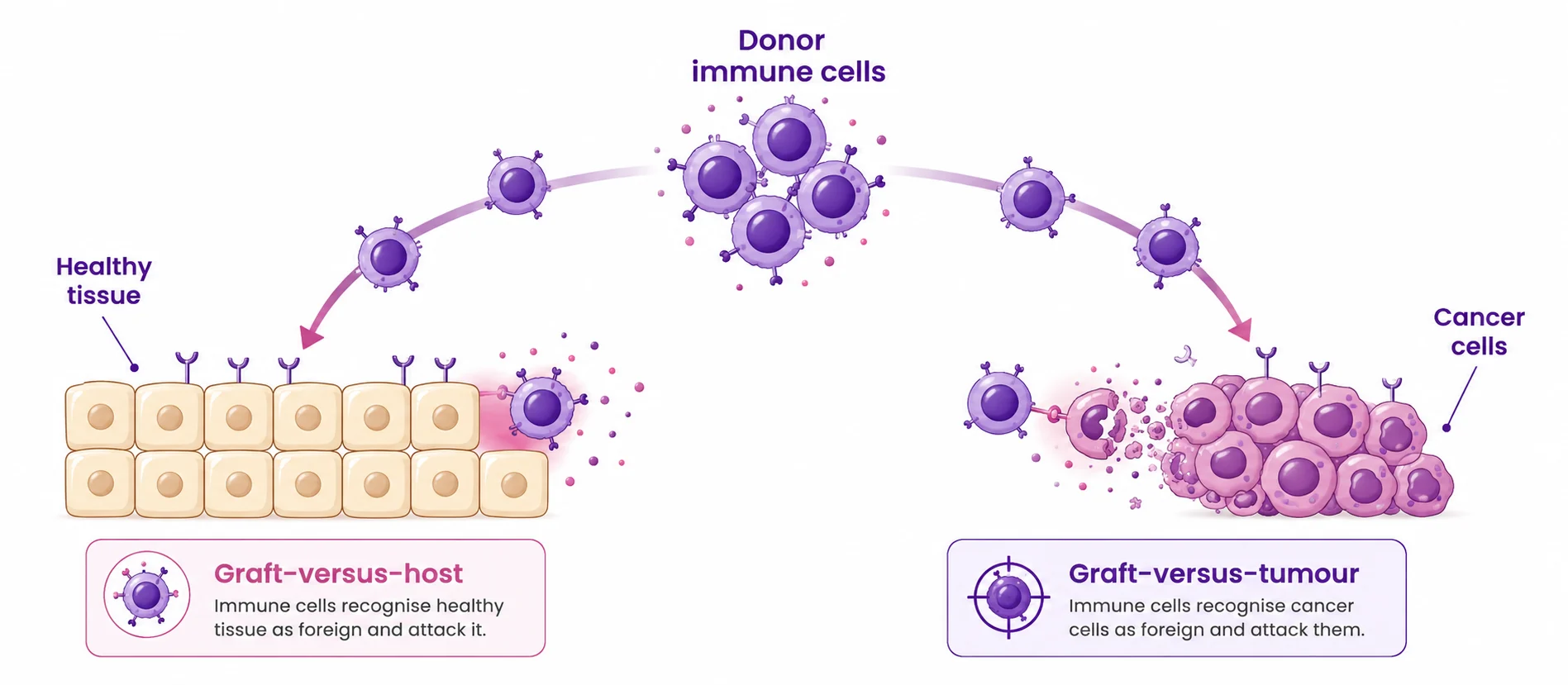
Graft-versus-host disease — and its other side
In a donor transplant, the arriving cells bring the donor's immune system with them. Sometimes that immune system treats the recipient's body as foreign — attacking the skin, gut or liver. This is graft-versus-host disease (GvHD): the complication families fear most and understand least. It can be mild, and it can be severe. It is monitored closely, and it is treatable.
Here is what is rarely explained. The same donor immune system that can attack your tissue also attacks any cancer cells left behind — the graft-versus-tumour effect, and a large part of why a donor transplant works at all. The goal of treatment is not to switch the donor's immune system off, but to hold it in the right place.
The same donor immune response can attack healthy tissue (GvHD) and residual cancer cells (graft-versus-tumour).
The other risks
Infection. The most immediate danger, and the reason for the isolation weeks.
Bleeding, while platelet counts are low.
Organ effects on the liver, kidneys, lungs or heart, from the conditioning treatment.
Fertility. Conditioning can affect fertility, often permanently. If this matters to you, raise it before treatment starts — options exist, but only beforehand.
Graft failure, where the new cells do not establish themselves.
Relapse. A transplant reduces the risk of the disease returning. It does not remove it.
About "success rates"
You will find success-rate figures quoted freely online, and you should treat almost all of them with suspicion. Outcomes vary enormously with the condition, the patient's age, the type of donor, and — above all — how well the disease had responded to treatment before the transplant. A twelve-year-old with thalassaemia and a matched sibling is in a completely different position from a sixty-year-old with leukaemia that has already returned once. A single headline percentage that ignores all of that is close to meaningless, and we are not going to put one on this page. A haematologist who has read your reports can give you figures that actually apply to you.
Recovery & follow-up
Recovery — and follow-up close to home
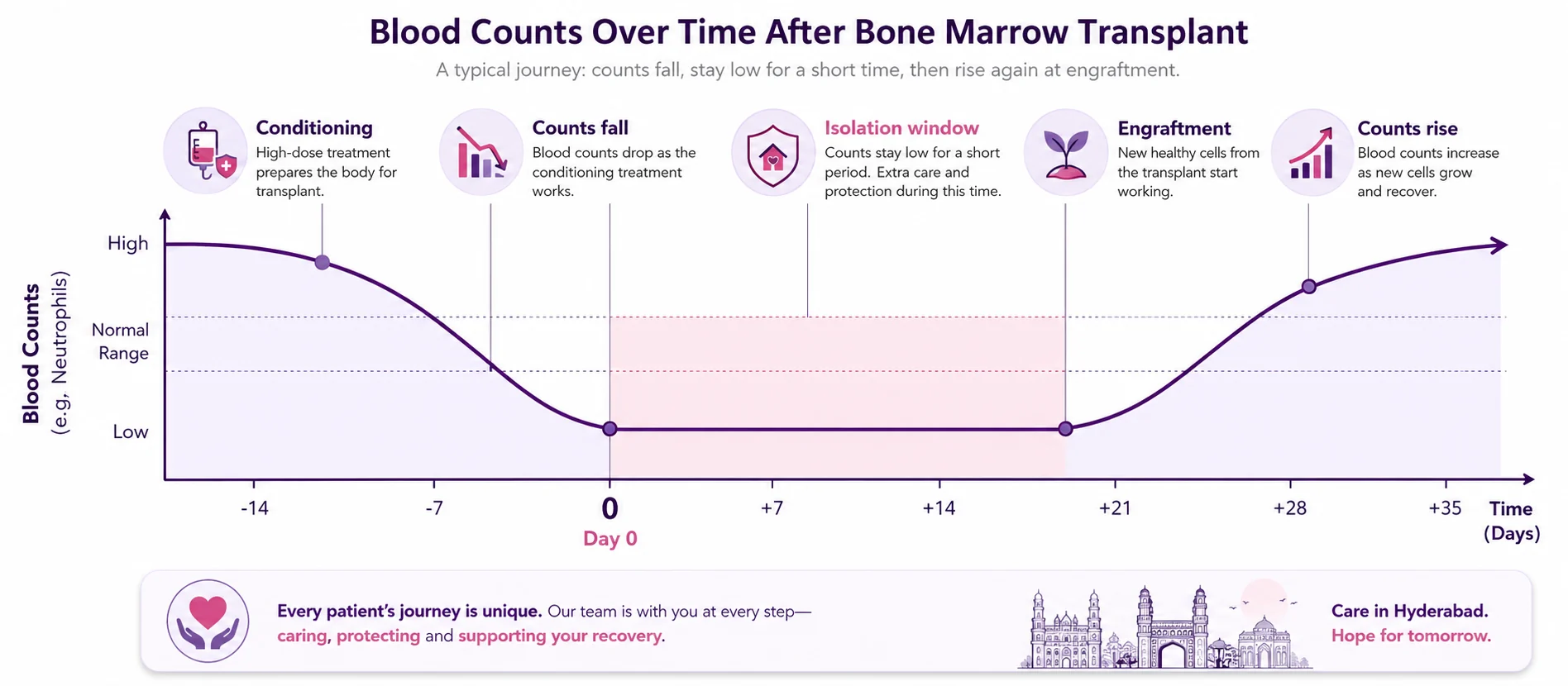
Why the isolation weeks happen
Families find the isolation period the cruellest part. It is not a rule made for the hospital's convenience. After conditioning, the patient has almost no infection-fighting white cells at all — for roughly two weeks, until the new stem cells engraft and start producing. In that window, an ordinary cold or a stomach bug carried in on a visitor's hands can become life-threatening. The isolation is what keeps them alive until their new marrow starts working. Video calls are almost always possible throughout.
Infection-fighting white cells fall to near zero after conditioning. The shaded window is why isolation is necessary.
Then comes the part nobody warns you about
Discharge is not the end. In the first year after a transplant, a patient typically needs thirty or more follow-up visits — blood counts, transfusions, medication reviews, checks for GvHD and infection — twice weekly at first, then weekly, then fortnightly, tapering over months. If you live in Hyderabad, that is inconvenient. If you live in Nizamabad, Suryapet, Vikarabad or Srikakulam, it is a serious problem: thirty-odd journeys, several hours each way, made by someone whose immune system is still rebuilding.
This is what CION's network is actually for. Your transplant happens at an accredited partner transplant centre in Hyderabad. Your follow-up — the counts, the transfusions, the supportive care — happens at your nearest CION centre, in your own town, reviewed by the same haematology team.
A single-site transplant hospital, however good, cannot offer you this. It is the one thing they cannot build.
Getting back to normal life. Most people are out of hospital within four to six weeks. The immune system takes months to rebuild, and the first three to six months at home mean real care around crowds, raw food and infection. Many people return to work, study and family life — how well and how quickly depends on your condition, your age, the type of transplant, and whether complications occur.
Cost should not decide whether a family even comes in. Under Aarogyasri and PMJAY, eligible treatment at empanelled centres may be supported, and private insurance is accepted cashless where applicable. Our counsellors help check eligibility and map out what you will actually pay — often a more workable picture than the advertised range suggests. If you cannot afford this, come in anyway and say so plainly: it is a more common conversation than you think.
9 clinics in Hyderabad · 35+ across Telangana & AP
Transplant in Hyderabad. Follow-up in your own town.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
With acute leukaemia, time is the one thing you cannot recover.
Before you commit to a transplant — or conclude nothing can be done — let CION's haematology team review your reports and tell you honestly whether you need one, and what it would really cost.
Asked quietly, usually after the doctor has left the room. Here are honest answers to the ones we hear most in Telangana.
“Is bone marrow taken from the spine?”
Fact: No. Nothing goes into the spine, ever. Most donors give stem cells through apheresis — blood drawn from one arm and returned through the other. Where marrow is collected, it is from the hip bone, under anaesthesia. This single belief is the biggest reason siblings refuse even to be tested.
“Will the donor be weak or paralysed for life?”
Fact: No. The body replaces donated stem cells within a few weeks. Donors return to normal activity within days of apheresis, and within a week or two after a marrow harvest — including heavy physical work. There is no permanent loss of strength and no paralysis.
“Does my family member actually need a transplant?”
Fact: Possibly not. Transplant is not standard for every blood cancer. Many lymphomas are treated without one, and most CML today is managed with a daily tablet at home. Before committing, ask for a second opinion with full molecular and cytogenetic review.
“We have no matching brother or sister — is there no hope?”
Fact: There is. A parent or a child is always at least a half-match, because you inherit half your HLA type from each parent. Half-matched (haploidentical) transplant is well established, and unrelated registries exist too. A family without a sibling match is not out of options.
“Why is the patient kept in isolation? Can we not visit?”
Fact: Isolation is the reason the transplant survives. After conditioning, the patient has almost no infection-fighting white cells for about two weeks. An ordinary cold carried in on a visitor's hands can become life-threatening. Restrictions ease once counts recover, and video calls are almost always possible.
“Can Ayurveda or home remedies treat it instead?”
Fact: Traditional practices bring comfort, but with acute leukaemia especially, time is the one thing that cannot be recovered — it progresses over days and weeks. Tell your haematologist about anything you want to continue; some are safe alongside treatment and some interfere.
“Will another person's marrow change who he is?”
Fact: No. What is transplanted is the blood-forming system — red cells, white cells and platelets. Brain, memory, character and identity are entirely unaffected. The only real change is that the recipient's blood group may gradually become the donor's, because blood group is decided by the marrow.
“Is a bone marrow transplant a surgery?”
Fact: No. There is no operation, no scalpel and no general anaesthesia for the transplant itself. The stem cells go in through a central line, much like a blood transfusion — the patient is awake and sitting up. What makes people unwell is the conditioning chemotherapy and the weeks of low immunity, not the transplant.
“Are they recommending this because he needs it, or because it is expensive?”
Fact: A fair question, and you are entitled to ask it out loud. A transplant is genuinely necessary for some and genuinely unnecessary for others — the difference lies in the molecular and cytogenetic reports. If something in you resists it, get a second opinion with a full review of those reports.
“Should we hide it? It could affect our daughter's marriage.”
Fact: Hiding a diagnosis isolates the person who most needs support and often delays treatment itself. There is nothing shameful about a blood cancer — it is not caused by anything anyone did. Telling people is usually what lets a family rally and get the patient treated sooner.
“Is cancer a punishment? Did we do something?”
Fact: No. Blood cancers arise from changes in cells — biology, not karma, not sin, not anything anyone did or failed to do. This belief makes people ashamed, makes them hide, and makes them delay. Nobody deserves a cancer, and nobody earns one.
“We cannot afford this — is there any point in even coming in?”
Fact: Come in anyway and say so plainly. It is worth knowing whether a transplant is even the right treatment, what the real cost is for your situation, whether your insurance or Aarogyasri applies, and what other support exists. Do not decide on a search result.
“Donating stem cells might give the donor cancer.”
Fact: No. Donating does not cause cancer and does not increase a donor's risk of it. The donor's marrow simply makes more cells to replace the ones given.
“A blood test now means she has agreed to donate.”
Fact: No. HLA typing is only a blood test. It commits nobody to anything — a person can be tested and still decide afterwards. Testing is information, not consent.
“A transplant will cure the cancer completely, so we won't need follow-up.”
Fact: A transplant reduces the risk of the disease returning but does not remove it, and the first year needs thirty or more follow-up visits. That follow-up is exactly what catches any problem early — and CION can do much of it at your nearest centre.
“He is too old for a transplant.”
Fact: Age alone does not decide it — fitness and organ function matter more. For some older patients a transplant is not the right choice; for others it is. Your haematologist assesses you individually rather than going by a number.
“A second opinion will offend our doctor or waste time.”
Fact: A second opinion is normal and welcomed in cancer care — it confirms the plan and gives you confidence. A doctor confident in the recommendation will not be offended. It is your money, and it is your family member's life.
“If there is no matched sibling, we should just wait and keep looking.”
Fact: With acute leukaemia, waiting has a cost. A parent or child is always a half-match, so a haploidentical route is usually available now rather than later. Start the blood tests and the conversation early — do not lose the window.
“The isolation ward means we are being kept away as punishment.”
Fact: It is protection, not punishment. During the weeks when immunity is near zero, keeping visitors and everyday infections out is what keeps the patient alive until the new marrow works. The team explains exactly when and how you can visit.
“Success rates online tell us what will happen to us.”
Fact: Treat online percentages with suspicion. Outcomes depend on the condition, age, donor type and how the disease responded before the transplant. A haematologist who has read your reports can give figures that actually apply to you — those are the only ones worth anything.
Why CION
Why CION for a bone marrow transplant
We are specific about what we do and what we coordinate, because you deserve straight information rather than marketing language. Your evaluation, haematology care, transplant decision and follow-up are led by CION's team; the transplant itself is performed at accredited partner transplant centres.
Indicative ₹8–15 lakh
Against a Hyderabad market that commonly quotes ₹10–35 lakh. Indicative — and we give you a real figure for your case.
A second opinion before you commit
Full molecular and cytogenetic review before any decision. Some people who arrive expecting a transplant turn out not to need one.
Follow-up in your own town
Thirty-plus visits in year one — do them at your nearest centre, not on a bus to Hyderabad while immunosuppressed.
A dedicated haematologist
Dr. Basudev Pokhrel — JIPMER and CMC Vellore. Not a general oncologist covering blood cancers as a sideline.
Every case to a tumour board
Haematology, medical oncology and pathology review your case together, not in sequence.
Care in accredited environments
The transplant is delivered at accredited partner transplant centres, to recognised protocols, with CION managing your case throughout.
Real stories · real courage
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
A transplant is not only a medical event. It is months of low immunity, long stretches away from home, and enormous strain on a family. These are part of the plan, not afterthoughts.
Nutrition counselling
Eating safely while immunity is suppressed — keeping weight and strength up through conditioning and recovery. Learn more
Psychological support
For the patient through weeks of isolation, and for the family carrying the fear and the cost. Learn more
Genetic counselling
Where an inherited condition such as thalassaemia is involved, or a family predisposition is suspected. Learn more
Rehabilitation
Rebuilding strength and stamina after weeks in a bed and months of low immunity. Learn more
Palliative & comfort care
Symptom and comfort support at any stage — alongside active treatment, not instead of it. Learn more
Financial counselling
Aarogyasri, PMJAY and cashless insurance guidance so cost never silently blocks care. Learn more
FAQ
Bone marrow transplant in Hyderabad — frequently asked questions
What does a bone marrow transplant cost in Hyderabad?
Bone marrow transplant in Hyderabad is commonly quoted between ₹10 lakh and ₹35 lakh depending on the centre and the type of transplant. At CION the indicative range is ₹8 lakh to ₹15 lakh: roughly ₹8–11 lakh for an autologous transplant using the patient's own stem cells, and roughly ₹11–15 lakh for an allogeneic transplant from a matched sibling donor. Half-matched and unrelated-donor transplants are assessed case by case. These figures are indicative and are not a quotation, and do not include family accommodation, travel, or medication after discharge.
Is a bone marrow transplant a surgery?
No. There is no operation, no scalpel and no general anaesthesia for the transplant itself. The stem cells are given as an infusion through a central line — a soft tube placed into a large vein — in much the same way as a blood transfusion. The patient is awake and sitting up, and it takes a few hours. What makes people unwell is the conditioning chemotherapy given in the days beforehand, and the weeks of low immunity afterwards, not the transplant.
Is bone marrow taken from the spine? Will the donor be paralysed or weakened?
No. Bone marrow is never taken from the spine, and donating does not cause paralysis or permanent weakness. Most donors today give stem cells through apheresis — blood is drawn from one arm, passed through a machine that separates out the stem cells, and returned through the other arm. There is no surgery and nothing goes into the back. When marrow itself is collected, it is taken from the hip bone, under anaesthesia, through a needle. The body replaces the donated cells within a few weeks, and donors return to normal work and normal life.
Does my family member actually need a bone marrow transplant?
Possibly not. Transplant is not the standard treatment for every blood cancer. Many people with lymphoma are treated with chemotherapy and immunotherapy alone and never need one. Most people with chronic myeloid leukaemia today take a daily tablet at home and rarely need a transplant. In acute myeloid leukaemia, whether a transplant is advised depends heavily on the genetic risk group of the disease and how it responds to first treatment. Before committing, it is entirely reasonable to ask for a second opinion with full molecular and cytogenetic review.
We have no matching brother or sister. Is there no hope?
There is. A full sibling has roughly a one in four chance of being a complete HLA match, so most families do not have one. But a parent or a child is always at least a half-match, because you inherit half of your HLA type from each parent. Half-matched, or haploidentical, transplant is now well established. A family with no sibling match is not out of options, and unrelated donor registries exist as well. Start with a haematology consultation rather than assuming the worst.
What are the types of bone marrow transplant?
There are four, named by where the stem cells come from. An autologous transplant uses your own stem cells, collected and given back. An allogeneic transplant uses cells from a fully HLA-matched sibling. A haploidentical transplant uses a half-matched parent or child. An unrelated-donor or cord-blood transplant uses cells from a registry donor or banked umbilical cord blood. The type determines the cost, the risks and the length of stay.
How does HLA matching work, and why is a sibling only a 1 in 4 chance?
Your HLA type — the set of markers a donor must match — comes in two halves, one inherited from each parent. Each parent has two halves to give, so there are four possible combinations a child can inherit. Two siblings match fully only when they happen to inherit the same combination, which is why the chance is about one in four. The same arithmetic explains why a parent or child is always exactly a half-match.
What is a haploidentical (half-matched) transplant?
A haploidentical transplant uses stem cells from a parent or a child, who is always at least a half-match because you inherit half your HLA type from each parent. It is now well established and performed routinely, and it is the reason a family with no matched sibling is not a family without a donor. If you have a living parent or an adult child, you have a potential donor.
Is bone marrow transplant covered under Aarogyasri or insurance?
Under Aarogyasri and PMJAY, eligible treatment at empanelled centres may be supported, subject to eligibility, and private insurance is accepted cashless where applicable. Coverage for transplant varies by scheme and by case, so the honest step is to have our counsellors check what applies to your specific situation and map out what you would actually pay, rather than assuming either that everything is covered or that nothing is.
Why is the patient kept in isolation? Can the family not visit?
Isolation is not a hospital rule made for convenience — it is the reason the transplant survives. The conditioning therapy clears the old bone marrow, so for roughly two weeks the patient has almost no infection-fighting white cells at all. In that window an ordinary cold, or a common stomach bug carried in on a visitor's hands, can become life-threatening. Once the new stem cells engraft and blood counts recover, restrictions ease. The team explains exactly when and how you can visit, and video calls are almost always possible throughout.
What is graft-versus-host disease (GvHD)?
In a donor transplant, the arriving cells bring the donor's immune system with them, and it can sometimes treat the recipient's body as foreign — attacking the skin, gut or liver. This is graft-versus-host disease. It can be mild or severe, it is monitored closely, and it is treatable. Importantly, the same donor immune system also attacks any remaining cancer cells (the graft-versus-tumour effect), which is a large part of why a donor transplant works at all.
Will receiving another person's bone marrow change who the patient is?
No. What is transplanted is the blood-forming system — the part of the body that produces red cells, white cells and platelets. A person's brain, memory, personality, character and identity are entirely unaffected. The one real change is that the recipient's blood group may gradually become the donor's, because blood group is determined by the marrow. It is a medical treatment for one organ system, not a transformation of the person.
Is donating stem cells safe? Does it affect fertility or cause cancer?
Donating stem cells is safe and well tolerated. It does not affect fertility, does not affect the ability to have children later, and does not cause cancer or increase a donor's risk of it. The body replaces donated cells within a few weeks. Most donors return to normal activity within days of apheresis, or within a week or two after a marrow harvest, including physical work.
How long does recovery take, and how many follow-up visits are needed?
Most people are out of hospital within four to six weeks, but the immune system takes months to rebuild. In the first year a patient typically needs thirty or more follow-up visits — blood counts, transfusions, medication reviews and checks for GvHD and infection — twice weekly at first, then weekly, then fortnightly. CION can carry out much of this follow-up at your nearest centre so you do not have to travel to Hyderabad repeatedly while your immune system is still recovering.
Can a person live a normal life after a bone marrow transplant?
Many people do return to work, study and family life. Recovery is gradual rather than sudden: most people are out of hospital within four to six weeks, but the immune system takes months to rebuild and follow-up continues for a year or more. During the first few months, crowds, raw food and infection risk have to be managed carefully. How well someone recovers depends on their condition, their age, the type of transplant and whether complications occur.
Does CION perform the transplant itself?
Your evaluation, haematology care, transplant decision and follow-up are led by CION's own team. The transplant itself is performed at accredited partner transplant centres in Hyderabad, under a formal arrangement, with the same haematology team managing your case throughout. This is stated plainly so you know exactly what CION delivers directly and what it coordinates — and it is also why routine follow-up can happen close to your home.
What is the success rate of a bone marrow transplant?
Outcomes vary enormously with the condition, the patient's age, the type of donor and — above all — how well the disease had responded to treatment before the transplant. A young person with thalassaemia and a matched sibling is in a very different position from an older person with leukaemia that has already returned. A single headline percentage that ignores all of that is close to meaningless. A haematologist who has read your reports can give you figures that actually apply to you.
Can Ayurveda or home remedies treat blood cancer instead of a transplant?
Traditional practices may bring comfort, and many families find real meaning in them. But with blood cancers — acute leukaemia in particular — time is the one thing that cannot be recovered, because it can progress over days and weeks, not months. Using traditional remedies instead of treatment spends exactly the window in which treatment works best. If you want to continue a traditional practice alongside medical treatment, tell your haematologist: some are safe alongside treatment and some interfere with it.
Explore
Explore blood cancer care at CION
Everything around blood cancer and transplant — diseases, treatments, tests and support. Tap any topic to read more.
Bring your reports, or come in for a fresh evaluation. Before you commit to a transplant, it is worth finding out whether you need one — and what it would really cost in your case. Consultations in Telugu, Hindi or English.
Medical disclaimer: This page provides general information about bone marrow (stem cell) transplant and is not a substitute for professional medical advice, diagnosis or treatment. Costs shown are indicative only and not a quotation. At CION, evaluation, haematology care, the transplant decision and follow-up are led by CION\'s team; the transplant itself is performed at accredited partner transplant centres. Always consult a qualified haematologist about your individual care. Content is periodically reviewed by CION\'s medical team.